Firstly, thanks very much for including both the afni_proc.py command and the QC images. That helps us understand things better from the start!
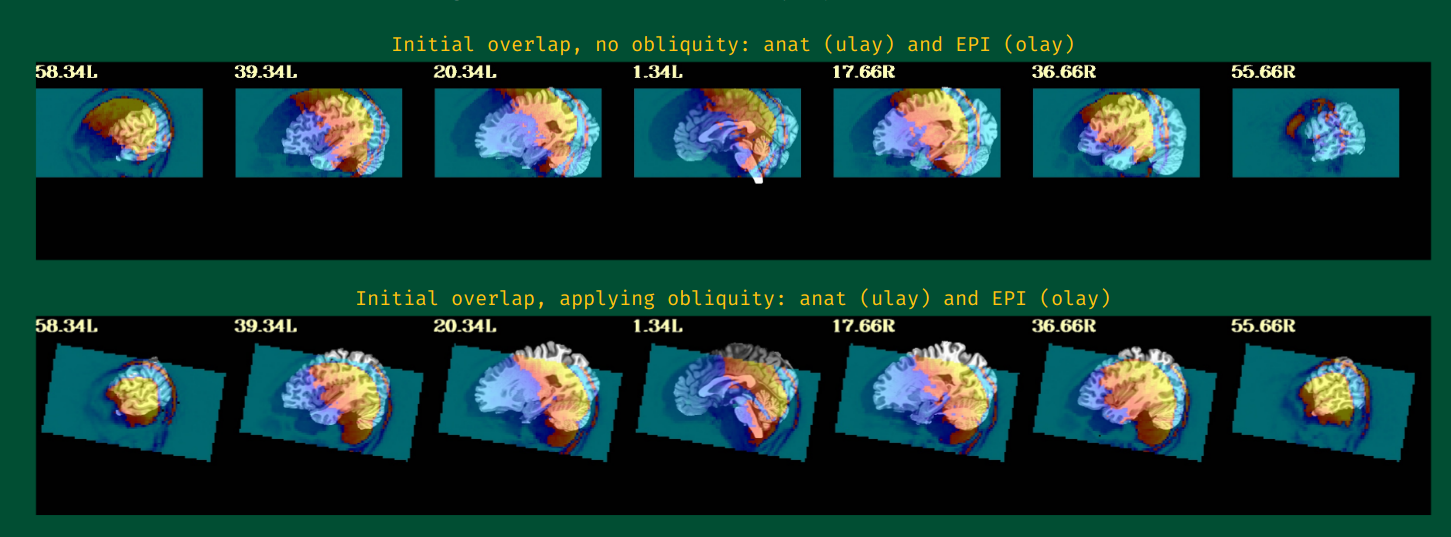
The initial, pre-alignment EPI-anatomical overlap is pretty good (second row of first image, "Initial overlap, applying obliquity..."). I think the poor alignment is probably due to two factors:
the options to control EPI-anatomical alignment were put into separate -align_opts_aea .. commands. I just checked, and while that doesn't pop up an error, the second of those is ignored. So that cost function and flip check aren't actually specified. Please just use a single, align_opts_aea command in the following way, like:
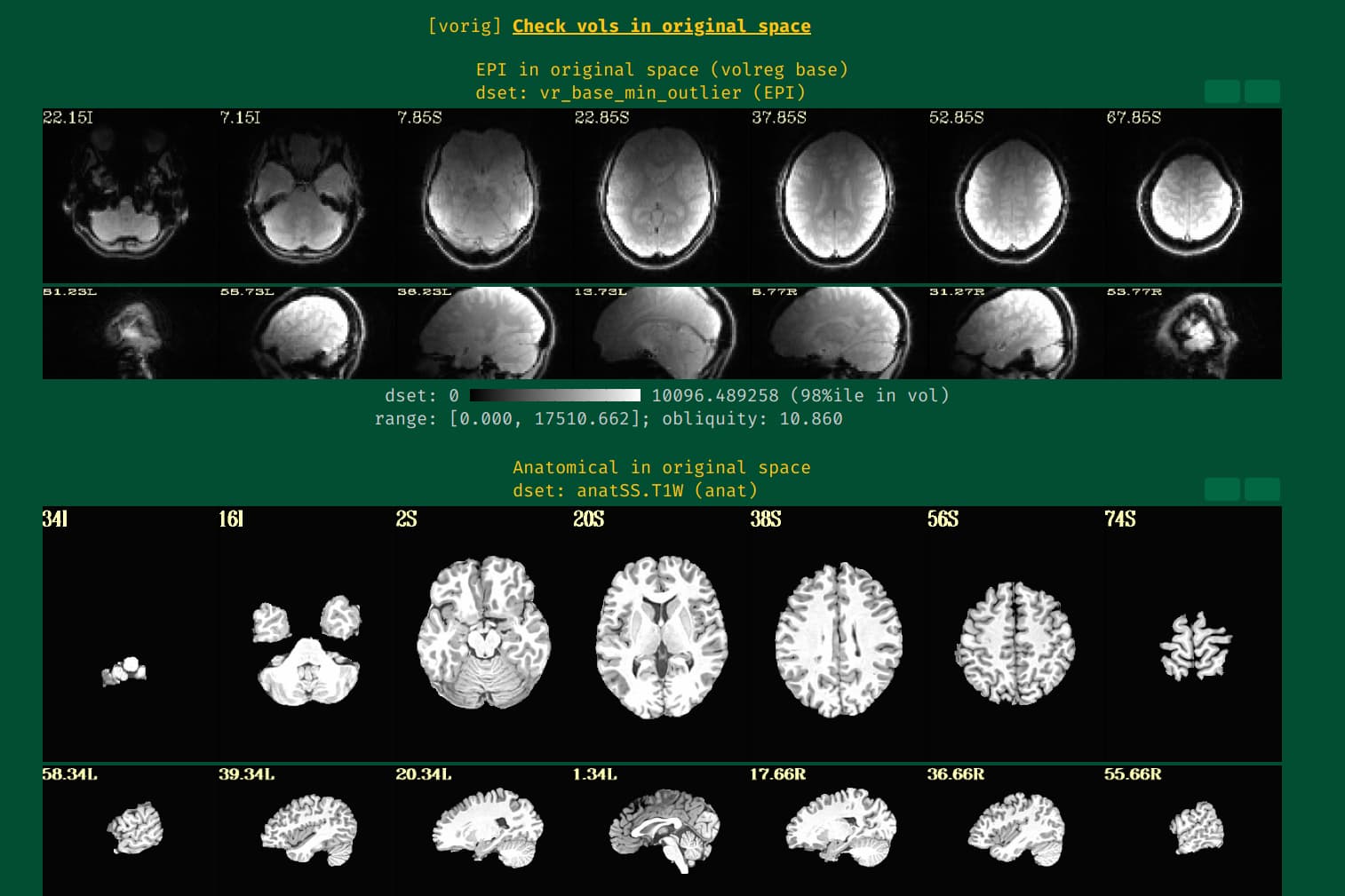
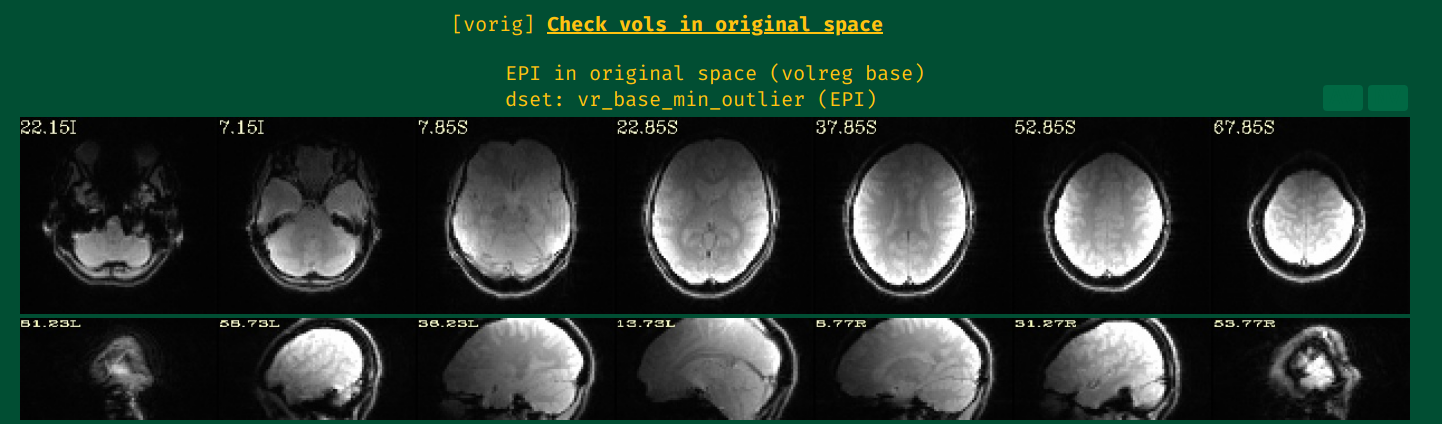
Also, the brightness inhomogeneity patterns across the EPI are pretty large (shown in vorig, top two rows, the EPI images). A couple years ago we added an option to try to help with that, so can you please add this to your afni_proc.py command:
-align_unifize_epi local \
I basically use this option in all human FMRI processing, as it usually either helps notably or has little effect, and I have never seen it lead to worse alignment.
Could you please adjust those things, and let us know how that does?
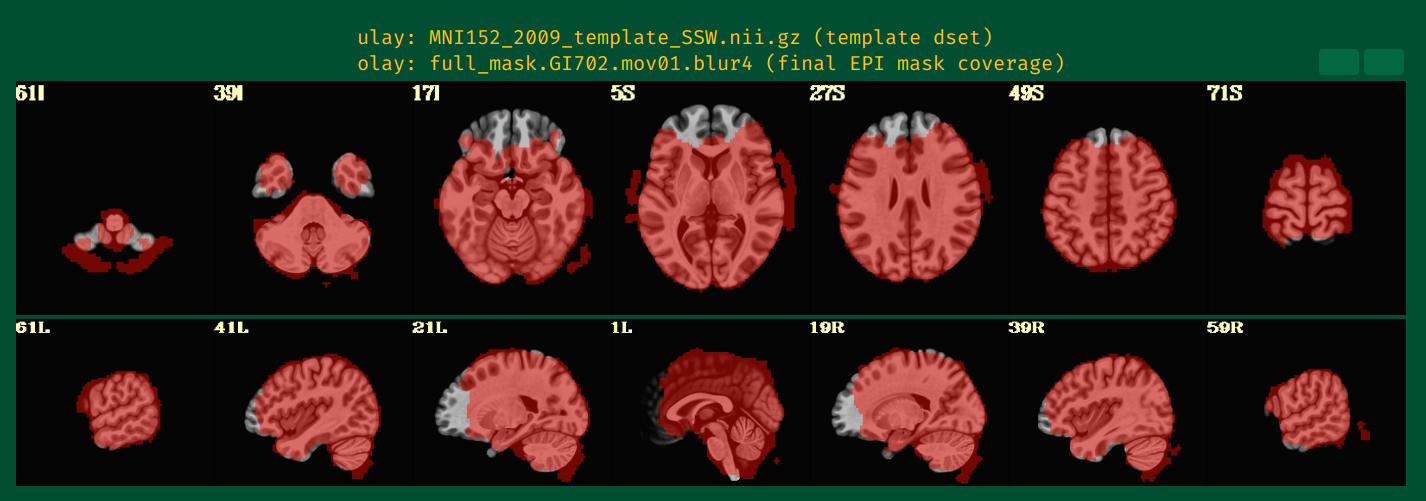
For all my subjects the full_mask looks good, however, for a single subject, 3dAutomask exclude voxels inside he brain...
I use multi-echo, the registration is for echo 1
-echo_times 12 31.7 51.4 -reg_echo 1
# create 'full_mask' dataset (union mask)
foreach run ( $runs )
3dAutomask -prefix rm.mask_r$run pb03.$subj.r$run.e$fave_echo.volreg+tlrc
end
# create union of inputs, output type is byte
3dmask_tool -inputs rm.mask_r*+tlrc.HEAD -union -prefix full_mask.$subj
I like to use -mask_apply epi and not anat or group.
I would look to the "vorig" images of the input EPI to look and see if there is dropout in those regions that don't appear in the automasking. Because this question is a continuation of a previous one, I can see that there deos appear to be a much lower signal in the frontral brain regions. I am not sure if this subject being shown here is the same as the one at the start of the thread, but it is possible that one subject might have more severe signal gradients/dropout than others. Can you post the image of the vorig EPI for this specific subject?
I see. That is specified in your AP command with -reg_echo 1, above.
Looking at AP's help for that option, it makes me wonder if using the second echo might be preferable? If the tissue contrast is good in the second echo, I wonder if the masking would be better?
-reg_echo ECHO_NUM : specify 1-based echo for registration
e.g. -reg_echo 3
default: 2
Multi-echo data is registered based on a single echo, with the
resulting transformations being applied to all echoes. Use this
option to specify the 1-based echo used to drive registration.
Note that the echo used for driving registration should have
reasonable tissue contrast.
Additionally or separately, you can control the automasking options that are applied to the reference EPI volume with this option:
-mask_opts_automask ... : specify extra options for 3dAutomask
e.g. -mask_opts_automask -clfrac 0.2 -dilate 1
This allows one to add extra options to the 3dAutomask command used
to create a mask from the EPI data.
Please see '3dAutomask -help' for more information.
You could specify a lower clfrac ("clipping fraction", see 3dAutomask's help), which would increase the mask size---that is, make it less sensitive to the changes. The default value is 0.5, I might try lowering to 0.4 to start---you can see what would work for this dataset prior to AP, with just running: 3dAutomask -prefix TEST1 -clfrac 0.4 DSET_EPI_ECHO1, for example. If that seemed good, then you would add this to AP:
-mask_opts_automask -clfrac 0.4
Figs. 14-15 here point out QC tools that will help you compare/evaluate TSNR across the brain quickly. Even if masking includes this region of hte brain, the TSNR might be problematically low there---that will be worth checking in the QC phase. You can also add your own specific ROIs to check in the QC with "-ROI_import ..`, as described here.
--pt
The
National Institute of Mental Health (NIMH) is part of the National Institutes of
Health (NIH), a component of the U.S. Department of Health and Human
Services.